Authors:
C. Adrian Austin MD MSCR
Snigda Jain MD MHS
Anand Iyer MD MSPH
Lauren Pollack MD MS
Angela Suen MD
Leah Witt MD
Louise Xu MD
Abebaw Yohannes MSc PhD
Editor:
Lauren Pollack MD MS
The purpose of this toolkit is to highlight key articles and select resources related to the care of older adults with chronic pulmonary disease or critical illness. The authors are members of the ATS Aging Interest Group who collectively care for patients across settings (ambulatory, acute care, intensive care unit) and have expertise and interest in integrating geriatrics principles into pulmonary and critical care medicine. The first version of the toolkit was published online in 2022, and the most recent update was in 2026.
Table of Contents:
4Ms Framework of an Age-Friendly Health System
Featured Section 1: Covid-19
Featured Section 2: Social Determinants of Health
Featured Section 3: Aging Physiology
The 4Ms Framework Applied to the Intensive Care Unit Setting
Critical Care: What Matters Most
Critical Care: Medications
Critical Care: Mentation and Mood
Critical Care: Mobility
The 4Ms Framework Applied to the Older Adult with Chronic Lung Disease
Pulmonary: What Matters Most
Pulmonary: Medications
Pulmonary: Mentation and Mood
Pulmonary: Mobility
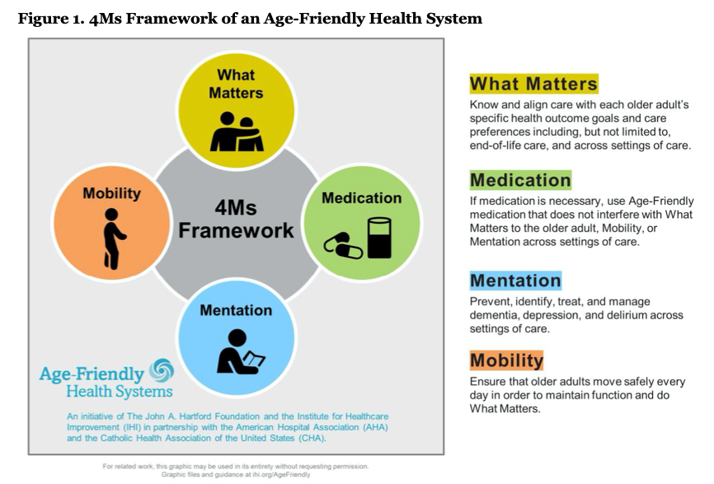
4Ms Framework of an Age-Friendly Health System
In the early 2000s, the Institute for Healthcare Improvement and the John A. Hartford Foundation created the 4Ms Framework (Figure 1) as part of the Age-Friendly Health System initiative to integrate elements of high-quality care for older adults across healthcare systems. The Age-Friendly Health System and the 4Ms Framework has been broadly adopted in hundreds of healthcare systems across the United States and internationally. The evidence-based 4Ms Framework – What Matters, Medications, M entation/Mood, and Mobility/Frailty – is associated with metrics of higher quality patient care such as patient satisfaction with care, shorter hospital length of stay, lower likelihood of hospital readmission, and fewer falls among older adults. The original research articles with accompanying summaries below as well as select review articles and resources are organized into components of the 4Ms framework. There are also three featured sections that fall outside this framework, focused specifically on: (1) the covid-19 pandemic, (2) social determinants of health, and (3) aging physiology.
More information: This article discusses practical recommendations for screening for delirium among critically ill older adults infected with COVID-19 given known poor outcomes associated with delirium in this population including prolonged mechanical ventilation, functional dependence, and persistent cognitive impairment. The authors review challenges to delirium screening related to the COVID-19 pandemic, such as reducing risk of virus transmission and family visitation restrictions, and potential solutions. Specific screening tools including the Confusion Assessment Method-ICU and the Intensive Care Delirium Screening Checklist are reviewed. Finally, the authors discuss challenges related to identifying delirium superimposed on dementia and screening in older adults with sensory impairments.
Bottomline: Given known poor outcomes associated with delirium among patients with critical illness, early recognition of delirium among older patients with COVID-19 is critical in order to reduce the burden of delirium. This article describes solutions to challenges related to delirium screening for critically ill older adults with COVID-19.
More information: This position statement of the American Geriatrics Society (AGS) reviews ethical considerations regarding how age is considered in the development of strategies for allocating scarce resources during the Covid-19 era and beyond. The AGS Ethics Committee developed these policy and clinical recommendations in collaboration with an interprofessional writing team of experts in ethics, law, nursing, and medicine. Topics reviewed include use of age as a determining factor or tiebreaker for research allocation, criteria with a differential impact on older adults, individual choices and advance directives, racial and ethnic disparities, scoring systems, and the need for post-pandemic review.
Bottom line: The AGS positions include avoiding use of age as a means of excluding anyone from care, considering the impact of social determinants of health and comorbidities, focusing on potential short-term (not long-term) outcomes, ensuring that resources allocation strategies are transparent and applied uniformly, and facilitating appropriate advance care planning among older adults.
More information: This commentary piece describes a frailty-based triage framework implemented in the Emergency Department at a single hospital to provide early geriatrics and palliative care assessments for older adults presenting to the hospital with confirmed or suspected COVID-19 infection. The Clinical Frailty Scale (CFS) was used to identify stable patients >= age 70 presenting to the Emergency Department with moderate or severe frailty. Patients with CFS scores of 4-6 were triaged to geriatric co-management, and those with scores of 7-9 to palliative care triage. Urgent palliative care consult in the ED was offered for unstable patients at high risk for intubation or decompensation. The authors report on processes of care and outcomes for 40 patients triaged between April and May of 2020.
Bottomline: The authors describe a novel framework in which frailty assessment is used to rapidly triage older adults with COVID-19 infection presenting to the Emergency Department to limited geriatrics and palliative care consultations.
More Information: This multicenter observational cohort study assessed frailty using the Clinical Frailty Scale in 1,564 adults (median age 74) hospitalized with COVID-19 across the United Kingdom (UK) and Italy. The study was intended to inform policy guidance, including National Institute for Health and Care Excellence (NICE) recommendations in the UK that used the Clinical Frailty Scale as a criterion to guide allocation of scarce resources during the COVID-19 pandemic. Increasing frailty was independently associated with higher in-hospital and early mortality, and frailty was a stronger predictor of outcomes than age or comorbidities.
Bottom Line: Frailty was more strongly associated with poor COVID-19 outcomes than age or comorbidities in hospitalized adults.
Featured Section 2: Social Determinants of Health
More Information: In this cohort study, the authors link a longitudinal survey of older adults with claims data to examine the association between socioeconomic disadvantage represented by dual-eligibility for Medicare and Medicaid and decline in the three PICS domains of function, cognition, and mental health after an ICU hospitalization. In results generalizable to more than 2 million ICU hospitalizations, they found that socioeconomically disadvantaged older adults developed a 28% greater count of disabilities in activities of daily living and mobility and a 9.8-fold greater odds of cognitive decline after an ICU hospitalization compared to their more advantaged counterparts despite accounting for many clinical characteristics including use of mechanical ventilation, frailty, multimorbidity, and pre-hospitalization functional and cognitive status.
Bottomline: Socioeconomic disadvantage is associated with functional and cognitive decline after ICU hospitalization. The study highlights the need to prioritize low-income seniors in rehabilitation and recovery efforts after ICU stay and to investigate differences in quality of acute and post-acute care that could underlie this disparity.
More information: In this systematic review of 25 articles, the authors summarized racial disparities in a variety of outcomes including mortality, ICU length of stay, discharge to long-term acute care, incidence of sepsis, and time to initiation of antibiotics across medical, surgical, cardiac, and neurological ICUs. Eight of the fifteen studies examining mortality, the most commonly studied outcome, reported a higher mortality rate among non-White patients compared to Whites although these differences were explained by controlling for age, comorbidities, and severity of illness. In two studies examining survival at hospital discharge after cardiac arrest and time to initiation of antibiotics respectively, worse outcomes among Blacks were explained by differences in the treating hospitals. Multiple studies demonstrated differences in palliative outcomes with non-White patients less likely to have comfort care orders placed, to have advanced care planning documentation, and to receive higher intensity of care than their White counterparts.
Bottomline: Racial differences exist in a breadth of ICU outcomes. While some of these are “explained” by differences in socioeconomic status, comorbidities, severity of illness, or treating hospitals, since these factors themselves are closely related to patient race, these could be underlying mechanisms and need to be investigated in future studies.
More Information: In this prospective cohort study of 239 ICU hospitalizations from 199 older persons, those living in socioeconomically disadvantaged neighborhoods, quantified by the Area Deprivation Index, a 100-point scale evaluating poverty, housing, and employment metrics, developed a 9% greater burden of disability in the 12 months following ICU discharge compared to those living in more advantaged neighborhoods. Disability burden was greater among those discharged home than those discharged to a facility. These findings highlight the need to investigate barriers to functional recovery among ICU survivors who live in disadvantaged neighborhoods.
Bottomline: Living in socioeconomically disadvantaged neighborhoods adversely affects functional recovery among older persons who survive ICU hospitalization.
More information: In this multicenter cohort study enrolling 1,040 survivors of shock and acute respiratory failure across 5 medical and surgical ICUs, the authors prospectively evaluated ICU-related long-term cognitive impairment using the Repeatable Battery for Assessment of Neuropsychological Symptoms (RBANS) score. They found that after adjusting for several illness related characteristics including sepsis, hypoxemia, duration of delirium, and coma, non-white race and lower education levels were associated with lower RBANS scores at 3 and 12 months following discharge from ICU hospitalization. Socioeconomic status assessed using the AHRQ socioeconomic index was not associated with cognitive impairment in this study.
Bottomline: After adjusting for hospital and illness characteristics, race and education but not socioeconomic index, assessed using a neighborhood socioeconomic index, is associated with long-term cognitive impairment following ICU hospitalization.
More information: In this retrospective cohort study, the authors examined trends in use of invasive mechanical ventilation (IMV) among 289,017 Medicare beneficiaries with advanced dementia hospitalized for pneumonia or septicemia between 2001 and 2014. The rate of IMV use was greater among Blacks, increasing from 8.6% to 21.8% between 2001 and 2014, compared with 3.7% to 12.1% for Whites. In adjusted models, Blacks had 34% greater odds of receiving IMV than Whites in the within-hospital model and 46% in the between-hospital model.
Bottomline: Among older adults with advanced dementia, racial differences exist in the use of mechanical ventilation both within the same hospital and between hospitals, suggesting individual as well as system-level factors driving its use.
Featured Section 3: Aging Physiology
More information: A retrospective cohort study comparing the fixed ratio definition of obstruction to LLN for the definition of obstruction in older adults and their associations with mortality. This longitudinal population-based study (Swedish National Study on Ageing and Care) followed older adults with repeated spirometry over ~6 years to examine the incidence and prognostic significance of airflow limitation defined either by fixed FEV₁/FVC ratio versus lower limit of normal (LLN). They found that incident airflow limitation was associated with a greater decline in FEV₁ regardless of diagnostic criterion. Airflow limitation defined by LLN, but not fixed ratio alone, was associated with increased mortality. Incidence rates and predictors differed substantially between criteria, highlighting important differences in epidemiology and prognostic relevance between diagnostic definitions of obstruction.
Bottom line: LLN is likely a better alternative than fixed-ratio in older adults as it has a lower risk of false-positivity without missing subjects at increased risk of mortality.
More information: This cross-sectional study analyzed data from the COPDGene cohort, including 10,131 adults (mean age 60 years) with a current or former smoking history, to compare clinical, functional, and imaging phenotypes using spirometric classifications defined by Global Lung Initiative (GLI) and GOLD criteria. Participants with GLI-defined normal spirometry were evaluated across GOLD spirometric categories. Although GOLD classified over 20% of individuals with GLI-defined normal spirometry as having respiratory impairment, these individuals did not demonstrate evidence of clinically meaningful respiratory disease by other measures.
Bottom line: Patients with GLI-defined normal spirometry but GOLD defined respiratory impairment did not have clinically meaningful respiratory disease, suggesting that the GLI may offer a more accurate measure of lung disease in older adults.
Review Article:
THE 4MS FRAMEWORK APPLIED TO THE INTENSIVE CARE UNIT SETTING
KEY POINTS:
- What Matters Most: Multiple studies have demonstrated that treatments provided to older patients with a critical illness are often incongruent with their care preferences. Eliciting individual care preferences from older patients and their health care proxies in order to ensure that the treatments received are aligned is a key component of delivering exceptional critical care. Potential strategies include providing structured and proactive family support through interprofessional teams, addressing both informational and emotional barriers to shared understanding about prognosis, and anchoring goals of care discussions on outcomes that patients value such as functional independence.
- Medications: Minimizing sedative and anti-psychotic medication exposure as able in critically ill older adults may improve patient outcomes. Thoughtful medication reconciliation during transitions in care from the ICU to acute care and at hospital discharge is important to prevent unnecessary polypharmacy.
- Mentation and Mood: Delirium is common among critically ill older adults and associated with long-term cognitive impairment; non-pharmacological prevention strategies such as clustered nursing care and early mobility may prevent or shorten the duration of delirium. Anxiety, depression, and post-traumatic stress disorder are also common, persistent, and often unrecognized consequences of critical illness for both patients and their families.
- Mobility: Early and consistent delivery of physical and occupational therapy during ICU hospitalization meaningfully improves functional recovery in older adults, yet remains substantially underutilized due to barriers such as hospital staffing and patient sedation level.
Select guidelines, and broad-based literature reviews:
- Ferrante LE, Chaudhuri D, Carayannopoulos KL, et al. Society of Critical Care Medicine Guidelines on Caring for Older Adults in the ICU. Crit Care Med. 2026 Mar 20. PMID: 41860322.
- Damluji AA, Forman DE, van Diepen S et al. Older Adults in the Cardiac Intensive Care Unit: Factoring Geriatric Syndromes in the Management, Prognosis, and Process of Care: A Scientific Statement From the American Heart Association. Circulation. 2020 Jan
- Brummel, N. E. & Ferrante, L. E. Integrating Geriatric Principles into Critical Care Medicine: The Time Is Now. Ann Am Thorac Soc 15, 518–522 (2018).
CRITICAL CARE – WHAT MATTERS MOST
More Information: This parallel-group randomized clinical trial evaluated a multidisciplinary palliative care intervention for family members of critically ill older adults across medical and surgical ICUs at two hospitals. The intervention used an automated, electronic health record-integrated mobile platform to capture family-reported palliative care needs, to coach ICU physicians on addressing those needs, and to trigger palliative care consultation when needs persisted. The intervention was feasible to implement and well-accepted by ICU clinicians. Despite higher rates of family meetings and palliative care consultations, the intervention did not significantly reduce family-reported needs, communication quality, goal-concordant care, or 3-month psychological distress compared with usual care.
Bottom Line: A needs-triggered, collaborative ICU palliative care model increased family meetings and specialty palliative care consultation, but did not improve measured family-centered outcomes, underscoring the difficulty of demonstrating benefit when care is concentrated among the most complex cases and the limitations of traditional ICU palliative care outcome measures.
More information: This prospective, multicenter, cluster-randomized controlled trial enrolled 875 relatives of patients hospitalized in 34 ICUs in France and compared standard care with a physician-driven, nurse-aided, support strategy for families following a decision to withdraw or withhold life support for their loved one. In the intervention group, three meetings were held with relatives: a family conference to prepare the relatives for the imminent death, an ICU-room visit to provide active support, and a meeting after the patient's death to offer condolences and closure. The intervention significantly decreased the prevalence of prolonged grief 6 months after the patient’s death, as well as the prevalence of PTSD symptoms and anxiety.
Bottom line: A proactive communication and support intervention provided by ICU physicians and nurses to relatives of dying patients may effectively reduce prolonged grief and other psychological harm.
More information: This web-based randomized trial among a national sample of 302 adult family members of people with COPD on supplemental oxygen assessed prognosis interpretation across 1 of 4 intensivist communication styles. Simulated intensivist styles were direct (control) or one of three indirect responses: indirect and comparative to other patients, indirect and descriptive of deterioration, and redirecting to values and goals. Compared to a direct response, participants perceived an indirect or redirecting response as more optimistic. Difference in belief (the difference between what the participant perceives the intensivist’s prognostic estimate to be and the participant’s own prognostic estimate) was optimistic for approximately three-fourths of participants regardless of intensivist response.
Bottom line: When families request information about prognosis, intensivists should convey the clinical team’s view using a simple, direct response.
More information: This review article examined observational and randomized trial evidence for advance care planning and palliative care interventions in both pre-hospital and hospital settings to avoid unwanted or non-beneficial ICU admission for patients with life-limiting illness.
Bottom line: For patients with chronic, life-limiting illness, discussions about goals of care should begin in the pre-hospital and outpatient setting and extend into the hospital setting, in advance of admission to the ICU.
More information: This multicenter, stepped-wedge, cluster-randomized trial involving 1420 patients with a high risk of death and their surrogates in five ICUs compared a multicomponent family-support intervention (featured by nurse-led communication and delivered by the interprofessional ICU team) with usual care. The intervention did not significantly affect the surrogates’ burden of psychological symptoms, but the surrogates’ ratings of the quality of communication and the patient- and family-centeredness of care were better. The length of stay in the ICU was shorter with the intervention, which was mediated by the shortened mean length of stay in the ICU among patients who died.
Bottom line: Family-support interventions could help surrogate decision-makers transition a patient’s treatment to goal-concordant, comfort-focused care, and in doing so shorten the dying process for those who face a dismal prognosis.
More information: This is the first multicenter, cluster-randomized controlled trial conducted among 34 French adult ICUs that studied the effectiveness of a multicomponent program in discomfort reduction. The program consisted of assessment of ICU-related self-perceived discomforts, immediate and monthly feedback to healthcare teams, and site-specific tailored interventions. There was a 7-point reduction of the overall discomfort score in the experimental group as compared to the control group, and the effect remained positive after adjustment for age, gender, ICU duration, mechanical ventilation duration, and type of admission.
Bottom line: Tailored interventions may decrease self-perceived discomfort in ICU patients.
More information: In this single-center, mixed-methods study, the authors used quantitative surveys and qualitative interviews across different types of ICUs and documented discordance in over half (53%) of 229 surrogates and 99 physicians involved in the care of 174 critically ill patients at high risk of death. The discordance was associated with both misunderstandings by surrogates of physicians’ assessment of prognosis and by surrogates holding different beliefs about a patient’s prognosis compared with what they perceived to be the physician’s assessment of prognosis. Discordant reasons for optimism among surrogates included loved-one’s need to maintain hope, beliefs that the patient had unique strengths unknown to the physician, and religious convictions.
Bottom line: Interventions are needed not only to improve the comprehensibility of prognostic information but also to attend to the emotional and psychological factors that influence surrogates’ prognostic expectations.
More information: This single-center prospective cohort study included 180 hospitalized patients aged 60 years or above with serious illnesses. A majority of respondents rated bowel and bladder incontinence (68.9%), requiring a breathing tube to live (67.2%), relying on a feeding tube to live (55.6%) and needing care from others all the time (53.9%) as health states the same or worse than death.
Bottom line: Hospitalized patients with serious illnesses often viewed states of serious functional debility as worse than death. This could inform future studies on patient-centered outcomes.
More information: This population-based cohort study evaluated sedative-naive ICU survivors aged ≥ 66 Ontario, Canada. Among ~250,000 ICU survivors, 6% filled a new sedative prescription within 7 days of hospital discharge, and more than half of these went on to refill prescriptions within 6 months. There was substantial interhospital variability in new sedative prescribing and hospital-level variation had a stronger association with new sedative use than patients’ comorbidity burden or admission diagnosis. Factors independently associated with new sedative prescriptions included discharge to a long-term care facility, inpatient geriatric or psychiatry consultation, invasive mechanical ventilation, and longer ICU length of stay.
Bottom line: Among sedative-naive older adult ICU survivors, 1 in 15 filled a new sedative prescription after hospital discharge, and over half of these became persistent users. Wide variation across hospitals, stronger than many patient-level factors, suggests an opportunity to improve patient care through sedation stewardship, improved discharge medication reconciliation, and coordinated post-ICU follow-up to reduce potentially avoidable long-term sedative exposure.
More information: This multicenter, pragmatic randomized clinical trial enrolled 2600 ICU patients aged ≥ 65 years with vasodilatory hypotension across 65 ICUs in the United Kingdom. Patients were randomized to a permissive hypotension strategy (target mean arterial pressure [MAP] 60–65 mm Hg) or usual care, in which vasopressor titration was left to clinician discretion. The permissive hypotension group had significantly lower vasopressor exposure, including shorter duration and lower total dose. At 90 days, mortality was 41.0% in the permissive hypotension group vs 44% in the usual care group (absolute risk difference −2.85%; 95% CI, −6.75% to 1.05%; p = .15). Adjusted analyses suggested a possible mortality benefit (adjusted OR 0.82; 95% CI, 0.68–0.98), although the primary unadjusted analysis was not statistically significant. Rates of serious adverse events, including acute renal failure and supraventricular arrhythmias, were similar between groups.
Bottom line: In older ICU patients with vasodilatory hypotension, targeting a lower MAP of 60–65 mm Hg reduced vasopressor exposure without increasing serious adverse events. The findings suggest permissive hypotension is likely safe and may modestly reduce vasopressor use.
More Information: This was a study of adults admitted for more than 24 hours to the ICU. Daily mental status was assessed and classified as either awake without delirium, delirious, or unarousable (comatose). A first-order Markov model with multinomial logistic regression analysis considered four possible next-day outcomes (i.e., awake without delirium, delirium, unarousable, and ICU discharge or death) and 11 delirium-related covariables. This model was used to quantify the association between opioid use, opioid dose, and delirium occurrence the next day. 4,075 adults had 26,250 ICU days. Severe pain was inversely associated with a transition to delirium (odds ratio [OR] 0.72; 95% confidence interval [CI], 0.53-0.97). Any opioid administration in awake patients without delirium was associated with an increased risk for delirium the next day [OR, 1.45; 95% CI, 1.24-1.69]. Each daily 10-mg intravenous morphine-equivalent dose was associated with a 2.4% increased risk for delirium the next day.
Bottomline: In this population, Opioid administration increased the odds of transitioning to delirium in a dose-dependent fashion.
More Information: This was a multicenter, randomized controlled trial that assigned mechanically ventilated ICU patients to no sedation vs light sedation (i.e., RASS -2 to -3) with daily interruption. Mortality at 90 days was 42% in the non-sedation group and 37% in the light sedation group (difference, 5.4 percentage points; 95% confidence interval [CI], -2.2 to 12.2; p = 0.65). The number of ICU-free days and of ventilator-free days did not differ significantly between the trial groups. The patients in the non-sedation group had a median of 27 days free from coma or delirium, and those in the sedation group had a median of 26 days free from coma or delirium.
Bottomline: Among mechanically ventilated ICU patients, mortality at 90 days did not differ significantly between those assigned to a plan of no sedation and those assigned to a plan of light sedation with daily interruption.
CRITICAL CARE – MENTATION AND MOOD
More information: This systematic review and network meta-analysis evaluated 12 non-pharmacological interventions for delirium prevention in older ICU patients (age ≥60 years) across 38 RCTs involving approximately 7,000 patients. Cluster nursing was the top-ranked intervention for reducing delirium incidence, delirium duration, and mechanical ventilation. Cluster nursing involves coordinating multiple care tasks into grouped intervals to minimize patient interruptions and protect rest. Interventions involving physical exercise ranked highest for reducing ICU length of stay and also significantly shortened delirium duration. Mortality rates did not differ meaningfully between intervention and control groups across the four studies that reported this outcome.
Bottom line: The findings highlight the central roles of nursing and physical exercise in ICU delirium prevention for older adults and underscores the need for standardized, evidence-based non-pharmacological protocols.
More information: This retrospective cohort study included approximately 700 adults age 65 years and older discharged from a single academic medical ICU. All patients had a health-system-affiliated primary care provider and were followed for one year. Only 25% completed a Medicare Annual Wellness Visit, a federally mandated visit that includes cognitive screening. Of those completing the Medicare Annual Wellness Visit, cognitive impairment was detected in only about 3%. A slightly higher prevalence (6%) was captured through routine encounter diagnosis codes or the electronic health record problem list. These proportions are far below the prevalence of cognitive impairment reported in prior observational studies.
Bottom line: The findings suggest a substantial burden of unrecognized post-ICU cognitive impairment and support calls for routine formal cognitive screening tools in this high-risk population.
More information: This prospective cohort study enrolled adult family caregivers paired with ICU patients (mean age 65 years) experiencing acute cardiorespiratory failure at a single U.S. tertiary-care center. PTSD symptoms were measured using the Impact of Events Scale-Revised at four time points: ICU admission, ICU discharge, and 3 and 6 months post-discharge. Latent class growth analysis identified two distinct symptom trajectories: a persistently high trajectory and a persistently low trajectory. Approximately two-thirds of caregivers fell into the persistently high group, with elevated PTSD symptoms at enrollment that remained elevated throughout the 6-month follow-up period.
Bottom line: The majority of family caregivers of critically ill patients experience persistently elevated PTSD symptoms from the time of ICU admission through 6 months post-discharge, suggesting that psychological distress in this population is established early and does not resolve spontaneously.
More information: The authors utilized prospectively collected cognitive data from 3,673 participants in the Mayo Clinic Study of Aging (age range 50–91 years, without dementia at enrollment), with ICU admissions ascertained from electronic medical records between 2004–2017. Among the sample, 372 participants had at least one ICU admission. Using linear mixed effects models, ICU admission was associated with significantly greater decline in cognitive function over time compared to those never admitted to the ICU. Declines were most pronounced in memory, attention/executive, and visuospatial domains. Among ICU patients who developed delirium, cognitive decline was significantly greater in memory and language domains compared to those without delirium.
Bottom line: ICU admission in older adults is independently associated with accelerated long-term cognitive decline across multiple domains, with delirium further compounding this trajectory. While causality remains difficult to establish given unmeasured confounding from underlying comorbidities, these findings reinforce the importance of delirium prevention in the ICU to preserve long-term cognitive function.
More information: This systematic review and meta-analysis searched five databases and identified 27 studies encompassing 2,880 adult ICU survivors. The Hospital Anxiety and Depression Scale-Anxiety subscale (HADS-A) was used in 81% of studies and served as the basis for pooled analysis. The prevalence of anxiety symptoms (HADS-A ≥8) was 32% at 2–3 months, 40% at 6 months, and 34% at 12–14 months post-ICU discharge. Psychiatric symptoms during the ICU admission and memories of in-ICU delusional experiences emerged as potential risk factors, while physical rehabilitation and ICU diaries showed potential benefit.
Bottom line: Approximately one in three ICU survivors experienced clinically significant anxiety symptoms that persisted throughout the first year of recovery, with little spontaneous improvement over time. Physical rehabilitation and ICU diaries warrant further investigation as targeted interventions for this underrecognized and persistent complication of critical illness.
More information: A randomized, double-blind, placebo-controlled trial, that assigned patients with acute respiratory failure or shock and hypoactive or hyperactive delirium to receive intravenous boluses of haloperidol, ziprasidone (maximum dose, 40 mg daily), or placebo. The use of haloperidol or ziprasidone, as compared with placebo, had no significant effect on the primary end point (odds ratios, 0.88 [95% CI, 0.64 to 1.21] and 1.04 [95% CI, 0.73 to 1.48], respectively).
Bottom line: Antipsychotics do not treat delirium in the ICU. it is our opinion that there may be a role for these drugs only to reduce severe agitation with the risk of patient harm.
More information: A prospective cohort study conducted from 1998 to 2013 with monthly assessments of disability. In the multivariable analysis, moderate cognitive impairment was associated with nearly a 20% increase in disability over the 6-month follow-up period (adjusted relative risk, 1.19; 95% confidence interval, 1.04-1.36), and minimal impairment was associated with a 16% increase in post-intensive care unit disability (adjusted relative risk, 1.16; 95% confidence interval, 1.02-1.32).
Bottom line: Among older adults, impairment in pre-intensive care unit cognitive status was associated with an increase in post-intensive care unit disability over the 6 months after critical illness; moderate cognitive impairment doubled the likelihood of a new nursing home admission.
More information: A multicenter prospective cohort study of critically ill patients aimed at estimating the prevalence of long-term cognitive impairment after critical illness. One out of four patients had cognitive impairment 12 months after critical illness that was similar in severity to that of patients with mild Alzheimer’s disease, and one of three had impairment typically associated with moderate traumatic brain injury. Long-term cognitive impairment affected both old and young patients, regardless of the burden of coexisting conditions at baseline. A longer duration of delirium was associated with worse long-term global cognition and executive function.
Bottom line: Cognitive impairment after critical illness is very common and in some patients persists for at least 1 year. Patients with a longer duration of delirium are more likely than those with a shorter duration of delirium to have cognitive deficits.
More information: This retrospective cohort study used the National Health and Aging Trends Study linked with Medicare claims (2011–2019) to examine days alive and at home in the 100 days after ICU discharge among community-dwelling ICU survivors age 65 years and older. The sample included 884 ICU admissions and the patients had a median age of 81 years. The median number of hours of in-hospital physical or occupational therapy delivered was about 1 hour per 6 days. In adjusted analyses, each additional hour of in-hospital rehabilitation was associated with 8% higher odds of spending more days at home in the 100 days after discharge.
Bottom line: In this nationally representative study of older ICU survivors, greater in-hospital physical and occupational therapy was independently associated with more days alive and at home in the 100 days following discharge, suggesting that investment in rehabilitation during ICU hospitalization may yield meaningful gains in this patient-centered outcome.
More information: This retrospective study assessed mobility and self-care trajectories among older adults (age 65 years and older) admitted to a medical ICU at a single tertiary academic center between November 2018 and May 2019. Of 302 eligible patients, 44% received physical or occupational therapy consults, and 32% of those had at least two visits allowing longitudinal score comparison. Among patients with repeated assessments, 75% showed demonstrated improved mobility and 58% showed improved Modified Barthel Index scores. However, 17% of potential therapy days were missed due to inadequate staffing or time, and 14% due to patient sedation or encephalopathy.
Bottom line: Among older ICU patients who received physical or occupation therapy, modest but meaningful improvements in mobility and self-care were achievable prior to floor transfer, yet fewer than half of eligible patients received therapy consults at all. Staffing constraints and patient sedation were the primary barriers to delivery.
THE 4MS FRAMEWORK APPLIED TO THE PATIENT WITH CHRONIC LUNG DISEASE
KEY POINTS:
- What Matters Most: Understanding what matters most entails eliciting patients’ values, preferences, and healthcare goals, as well as how these priorities are weighed when healthcare decisions involve trade-offs. For older adults with chronic lung diseases such as ILD and COPD, early integration of specialty palliative care may improve outcomes and better align treatment with what matters most to patients.
- Medications: When prescribing medications for older adults with chronic lung disease, clinicians should carefully consider the risk of adverse effects, polypharmacy, medication costs, and the patient's ability to properly administer medications, particularly inhaled therapies. Beyond safety and feasibility, it is worth reflecting on whether the endpoints used to establish drug efficacy in clinical trials align with what matters most to the individual older adult.
- Mentation and Mood: Cognitive impairment, psychological distress, and social isolation are highly prevalent among older adults with chronic lung disease and are frequently underrecognized and undertreated in the ambulatory pulmonary setting. These conditions directly affect treatment adherence, self-management capacity, and caregiver burden, underscoring the importance of awareness and screening in clinical practice. Pulmonary rehabilitation may offer one avenue for addressing these concerns, as emerging evidence suggests it may improve cognition in patients with stable COPD, though the evidence base for most interventions in this space remains limited.
- Mobility: Frailty and mobility impairment are highly prevalent among older adults with chronic lung disease and carry important prognostic implications. Pulmonary rehabilitation is an effective yet underutilized intervention that can improve functional outcomes and may even reverse frailty status older adults with COPD.
Select guidelines, broad-based literature reviews, and web resources:
- Pulmonary Disease in the Older Adult. Clinics in Geriatric Medicine. Volume 41 Issue 4 p463-632. Edition edited by Leah J Witt, MD and C. Adrian Austin MD MSCR.
- Celli BR, Fabbri LM, Yohannes AM et al. A person-centered clinical approach to the multimorbid patient with COPD. Eur J Intern Med. 2025 Oct:140:106424. PMID: 40803921
- USPTF Lung Cancer Screening Recommendations
- Should I Screen? (University of Michigan)
- COPD Foundation
- Live Better
More Information: This mixed-methods study evaluated a palliative care-ILD collaborative care pilot program. Thirty-one patients (48% with IPF) were co-managed by palliative care and ILD teams. Nearly half received all palliative care via telehealth. Palliative care co-management was associated with advance care planning note completion rising from 3% to 100%, advance directive completion from 23% to 36%, and POLST form completion from 0% to 36%. Over half of patients were prescribed opioids, predominantly short-acting agents for episodic dyspnea. Patients reported perceiving the palliative care team as supportive and patient-centered and reported improved symptoms and illness understanding.
Bottom Line: Palliative care co-management for patients with moderately severe ILD is a promising approach to improving patient care.
More Information: This retrospective study using administrative health data from Alberta, Canada examined nearly 3,000 patients with IPF who were hospitalized and died (2012-2018). Patients were divided into three groups: those receiving multidisciplinary collaborative (MDC) care incorporating early integrated palliative care, specialist care (SC) from a pulmonologist, or non-specialist care (NSC). receiving multidisciplinary collaborative care were more than three times as likely to have received antifibrotic therapies, had nearly twice the odds of receiving pulmonary rehabilitation and were more likely to have received opioids. They also had lower total healthcare costs in the last 3 months of life primarily driven by fewer hospitalizations and emergency department visits, and were less likely to die in the hospital.
Bottom Line: An integrated palliative approach in ILD was associated with improved quality of end-of-life care and significantly reduced healthcare costs compared to conventional care.
More Information: This was a randomized, double-blind, placebo-controlled trial enrolling outpatients with COPD and moderate to very severe chronic breathlessness (mMRC grades 2–4) despite optimal treatment, recruited from a pulmonary rehabilitation center between 2016 and 2019. Participants received either 10 mg oral sustained-release morphine or placebo twice daily for 4 weeks, with the option to increase to three times daily. There were 124 participants (mean age ~66). The group receiving morphine had CAT scores about 2 points lower in the morphine compared to the placebo group. Overall breathlessness was unchanged, though worst breathlessness improved in those with mMRC grades 3–4. Nine percent of morphine participants withdrew due to adverse effects compared to 2% in the placebo group, with no morphine-related hospitalizations or deaths.
Bottom Line: Regular low-dose oral sustained-release morphine improved disease-specific health status in patients with COPD without causing serious adverse effects, with the greatest breathlessness benefit seen in those with more severe dyspnea.
More Information: This formative evaluation assessed early palliative care needs among 10 patients with moderate to very severe COPD and 10 family caregivers using validated surveys and semi-structured interviews. Patients had a mean age of 60 years and 70% were male. Overall, 30% reported poor quality of life, 45% reported anxiety, 25% reported depressive symptoms, and 40% reported social isolation. All participants responded positively to a standardized description of early palliative care and were receptive to its integration as early as moderate stage. Early palliative care needs including strategies for coping with COPD, managing both emotional symptoms and respiratory symptoms, illness understanding, and prognostic awareness.
Bottom Line: Patients with moderate to very severe COPD and their family caregivers found early palliative care acceptable and felt it should be integrated before end-stage disease, with coping and emotional symptoms identified as the highest priority needs.
Select Review Articles:
- Chen E, O'Mahony S. Palliative care in the older adult with advanced lung disease. Ann Palliat Med. 2025;14(1):90-100. PMID: 39963761.
- Holland AE, Spathis A, Marsaa K, et al. European Respiratory Society clinical practice guideline on symptom management for adults with serious respiratory illness. Eur Respir J. 2024;63(6):2400335. PMID: 38719772.
- Iyer AS, Sullivan DR, Lindell KO, et al. The Role of Palliative Care in COPD. Chest. 2022;161(5):1250-1262. PMID: 34740592.
- Sullivan DR, Iyer AS, Enguidanos S, et al. Palliative Care Early in the Care Continuum among Patients with Serious Respiratory Illness: An Official ATS/AAHPM/HPNA/SWHPN Policy Statement. Am J Respir Crit Care Med. 2022;206(6):e44-e69. PMID: 36112774
- Kreuter M, Bendstrup E, Russell AM, et al. Palliative care in interstitial lung disease: living well. Lancet Respir Med. 2017;5(12):968-980. PMID: 29033267.
More Information: This quasi-experimental difference-in-differences study used data from the 2021–2024 National Health Interview Survey to evaluate the impact of the Inflation Reduction Act's 2024 prescription drug provisions on cost-related medication nonadherence and healthcare-related financial strain. The study compared Medicare Part D beneficiaries aged 62–67 years (n=1,454) to a privately insured comparator group (n=3,797), excluding those with preexisting cost protections. The 2024 provisions included elimination of the 5% catastrophic coverage coinsurance requirement, effectively capping annual out-of-pocket drug costs at ~$3,300, and expansion of full low-income subsidies. Following implementation, cost-related medication nonadherence declined significantly among Medicare beneficiaries relative to comparators (-5 percentage points), with an even larger effect observed among those with multiple chronic conditions (-8 percentage points). However, no meaningful change was observed in healthcare-related financial strain.
Bottom Line: The Inflation Reduction Act's 2024 prescription drug provisions were associated with a meaningful reduction in cost-related medication nonadherence among Medicare beneficiaries in their first year of implementation, particularly among those managing multiple chronic conditions.
More Information:This retrospective multi-center study aimed to evaluate the tolerability and safety of antifibrotic medications (pirfenidone and nintedanib) in patients of age 75 years or older with idiopathic pulmonary fibrosis (IPF) in a real-world setting. Researchers reviewed medical records of 284 older and 446 younger (age < 75 years) IPF patient. Older patients experienced significantly more adverse events (63% vs. 55%) and dose reductions (27% vs. 18%) than younger patients, with the most common side effects being weight loss, loss of appetite, and nausea. Discontinuation rates were similar between the two groups.
Bottom Line:While older adults with IPF on antifibrotics had more side effects and required more dose reductions than younger patients, they were able to stay on treatment at similar rates, suggesting antifibrotics remain a viable option in this population with appropriate monitoring.
More Information: This retrospective study analyzed 614 consecutive patients (median age 65 years) treated for Mycobacterium avium complex pulmonary disease between 2009 and 2020 at a tertiary referral hospital in Korea. The primary outcomes were long-term treatment success, defined as negative culture conversion sustained for more than 12 months, and adverse drug reactions. Both median treatment duration and long-term treatment success declined significantly with increasing age, while adverse drug reactions increased. Among patients of age 80 years or older, only 21% had long-term treatment success. About 1 in 5 patients age 80 years or older discontinued treatment due to adverse drug reaction.
Bottom Line: In patients with Mycobacterium avium complex pulmonary disease, older age is associated with worse treatment outcomes and higher rates of adverse drug reactions. Patient education about realistic treatment expectations and potential side effects, as well as consideration of reduced-intensity, individualized approaches when treatment is pursued, is particularly important in older adults.
More Information:This cross-sectional study aimed to evaluate peak inspiratory flow rates among COPD patients using dry powder inhalers (DPIs) with varying internal resistances. A total of 138 patients (median age 72) from a medical center in Taiwan were included. While most patients achieved optimal peak inspiratory flow rates across devices, a substantial proportion (42%) demonstrated improper inhalation, particularly excessive peak inspiratory flow rates with low-resistance devices. Suboptimal or insufficient peak inspiratory flow rates were less common overall but were more frequently observed in patients older than 75 years when using medium-high resistance inhalers. These findings indicate that both excessive and inadequate inspiratory effort are clinically relevant and vary depending on device resistance.
Bottom Line:Improper peak inspiratory flow rates, especially excessive inhalation with low-resistance dry powder inhalers, are common in older adults with COPD, highlighting the need for device-specific assessment and patient training.
More Information:This observational, single-center cohort study aimed to determine the prevalence of peak inspiratory flow rate discordance, defined as suboptimal inspiratory flow for a patient’s prescribed dry powder inhaler (DPI), and identify associated clinical factors in stable COPD patients. The study included 66 patients (median age 70). Overall, 40% of participants were discordant with their prescribed DPI, indicating inadequate inspiratory effort during typical use. Female sex was the only factor consistently associated with lower peak inspiratory flow rate, while shorter height correlated with reduced peak inspiratory flow rate for low–medium resistance devices. No significant relationship was found between PIFR measured and standard spirometry, suggesting device-specific assessment is necessary.
Bottom Line:A substantial proportion of older adults with COPD may not generate sufficient inspiratory flow for their prescribed DPI, underscoring the importance of individualized device selection and consideration of peak inspiratory flow rate assessment.
PULMONARY – MENTATION AND MOOD
More Information: This was a cross-sectional study examining the prevalence of and characteristics associated with social isolation and loneliness among community-dwelling adults age 50 years and older with COPD enrolled in the Health and Retirement Study (2016-2018). The study included about 10,000 participants. Those with COPD had significantly higher rates of social isolation (16%) and loneliness (18%) compared to those without COPD (11% prevalence of both social isolation and loneliness). Those with COPD who used supplemental oxygen had higher rates of both social isolation and loneliness (20% and 22%, respectively).
Bottom Line: Adults with COPD, particularly those using supplemental oxygen, experience substantially higher rates of social isolation and loneliness than the general population, highlighting the need for routine screening and targeted interventions in this group.
More Information:This was a qualitative study aimed at identifying barriers and opportunities to addressing psychological distress among patients with COPD. The authors conducted semi-structured interviews with 31 participants, including clinicians and other healthcare staff, patients, and caregivers, at two pulmonary clinics.
Nearly all pulmonary clinicians recognized psychological well-being as a critical unmet need. However, they also reported insufficient training, limited resources, competing priorities around physical symptom management, and a lack of cultural support within the clinic setting to address psychological concerns. Patients and caregivers, by contrast, strongly desired integration of psychological care into routine pulmonary visits. Clinicians and patients both identified adding or training non-physician pulmonary staff to screen and provide initial management of psychological distress as a highly acceptable solution.
Bottom Line:Despite near-universal recognition among pulmonary clinicians that psychological distress represents an unmet need for many patients with COPD, structural and cultural barriers in the ambulatory pulmonary setting may prevent routine identification and management.
More Information: This was a prospective study aimed at examining cognitive recovery following an acute exacerbation of COPD and the effect of pulmonary rehabilitation on cognition in stable COPD. The study included 45 patients who had been hospitalized for an acute exacerbation and 67 patients with stable COPD who completed pulmonary rehabilitation, measuring cognitive function, health status, physical function, and psychological well-being at baseline and at 6 weeks. The median age was 68 years in the group that had been hospitalized for exacerbation and 69 in the group with stabled COPD. In both groups, over half of participants had cognitive impairment of at least mild severity based on the Montreal Cognitive Assessment. Among those recovering from an acute exacerbation, cognition did not improve over 6 weeks despite improvements in all other clinical outcomes. In the stable COPD group, those with cognitive impairment at baseline showed significant improvement in cognitive scores following pulmonary rehabilitation.
Bottom Line: Cognitive impairment is highly prevalent among patients with COPD. Pulmonary rehabilitation is associated with improved cognition in people with stable COPD and baseline cognitive impairment.
More Information: This was a prospective cohort study aimed at examining whether impaired lung function or lung disease in midlife is associated with increased risk of dementia and mild cognitive impairment later in life. Researchers followed 14,184 Atherosclerosis Risk in Communities study participants who underwent spirometry at baseline (1987–1989) through 2013. Both restrictive and obstructive lung disease were associated with higher odds of dementia or mild cognitive impairment compared to those without disease or respiratory symptoms, with restrictive impairment showing a stronger association. Findings held among nonsmokers and were present for both Alzheimer's disease-related and cerebrovascular etiologies.
Bottom Line: Midlife lung disease and reduced lung function are associated with modestly increased odds of dementia and MCI later in life, independent of smoking status.
Select Review Articles:
- Yohannes AM, Newman M, Kunik ME. Psychiatric Collaborative Care for Patients With Respiratory Disease. Chest. 2019 Jun;155(6):1288-1295. PMID: 30825443
- Hanada M, Tanaka T, Kozu R et al. The interplay of physical and cognitive function in rehabilitation of interstitial lung disease patients: a narrative review. J Thorac Dis. 2023 Aug 31;15(8):4503-4521. PMID: 37691666
More Information: This was a cross-sectional online survey of 69 patients with physician-confirmed interstitial lung disease, aimed at eliciting patient perspectives on functional capacity and self-management. Researchers assessed breathlessness, cough, frailty, and health-related quality of life using standardized instruments. Functional limitations were substantial, with 73% reporting mobility impairment, 77% reporting limitations in daily activities. Oxygen use was common in the sample (51% during exertion, 26% at rest). Nearly one in five were classified as frail based on the Clinical Frailty Scale.
Bottom Line: People living with interstitial lung disease experience substantial functional decline, with the majority reporting mobility impairment and very limited daily activity. The authors suggest a multidimensional approach to care that combines early antifibrotic initiation with personalized symptom management and comprehensive rehabilitation.
More Information: This was a prospective cohort study aimed at describing the prevalence of physical frailty and its prognostic impact across a spectrum of fibrotic interstitial lung disease. Researchers followed 463 patients (mean age 68 years) at a single interstitial lung disease program from 2015 to 2020, classifying participants as non-frail, pre-frail, or frail using modified Fried physical frailty criteria. The majority were pre-frail (56%) or frail (26%), with only 18% classified as non-frail. Both pre-frail and frail patients had a markedly higher risk of death compared to non-frail patients independent of age, sex, lung function, and diagnosis.
Bottom Line: Physical frailty is highly prevalent in patients with fibrotic interstitial lung disease and is independently associated with a substantially increased risk of death, suggesting frailty assessment may offer important prognostic value beyond existing risk scores.
More Information: This retrospective observational study examined whether initiation of pulmonary rehabilitation within 90 days of hospital discharge for COPD was associated with improved survival among older adults enrolled in Medicare fee-for-service plans. The sample included nearly 200,000 older adults hospitalized for COPD, of whom fewer than 2% initiated pulmonary rehabilitation within 90 days of discharge. Early initiation of pulmonary rehabilitation was significantly associated with a lower risk of death at one year compared to later or no initiation, and a greater number of sessions completed within the first 90 days was also associated with improved survival.
Bottom Line: Among older adults who had been hospitalized for COPD, early initiation of pulmonary rehabilitation was associated with substantially lower one-year mortality, yet few patients initiated it within 90 days of discharge. These results reinforce the importance of developing more effective strategies for increasing participation in rehabilitation.
More Information: This prospective cohort study was aimed at determining the prevalence of frailty and geriatric conditions in 50 patients age 65 years and older with idiopathic pulmonary fibrosis at a single center. Researchers assessed frailty using the Fried Frailty Phenotype alongside measures of functional status, geriatric conditions, and symptoms. Nearly half of participants were classified as frail and 40% had two or more geriatric conditions. Frailty was associated with lower lung function, shorter six-minute walk distance, higher symptom burden, and greater comorbidity.
Bottom Line: Frailty and geriatric conditions are highly prevalent in older adults with idiopathic pulmonary fibrosis and are associated with both objective and subjective markers of disease severity.
More Information: This was a prospective cohort study aimed at determining the prevalence of frailty among patients with stable COPD and examining the association between frailty and pulmonary rehabilitation completion and outcomes. Researchers assessed frailty using the Fried criteria in about 800 patients (mean age 70 years) before and after pulmonary rehabilitation. One in four patients were frail, and frail patients had double the odds of not completing the program, most often due to exacerbation or hospitalization. However, among those who completed rehabilitation, those with baseline frailty demonstrated consistently greater improvements in breathlessness, exercise performance, physical activity, and health status. Nearly two-thirds (61%) of previously frail patients who completed pulmonary rehabilitation no longer met frailty criteria after the program.
Bottom Line: While frailty is common among patients with COPD and significantly increases the risk of not completing pulmonary rehabilitation, patients who are frail and do complete it respond favorably and may experience reversal of their frailty status.
Select Review Articles and Guidelines:
- Maddocks M, Brighton LJ, Alison JA et al. Rehabilitation for People with Respiratory Disease and Frailty: An Official American Thoracic Society Workshop Report. Ann Am Thorac Soc. 2023 Jun 1;20(6):767-780. PMID: 37261787
- Rochester CL, Alison JA, Carlin B et al. Pulmonary Rehabilitation for Adults with Chronic Respiratory Disease: An Official American Thoracic Society Clinical Practice Guideline. Am J Respir Crit Care Med . 2023 Aug 15;208(4):e7-e26. PMID: 37581410