Author
María A. Rodríguez-Santiago, MD 1
Elsie Cruz-Cuevas, MD 1
Mark A. Vergara-Gómez, MD 2
1University of Puerto Rico, School of Medicine, Internal Medicine Department
2University of Puerto Rico, School of Medicine, Division of Pulmonary and Critical Care Medicine
Case
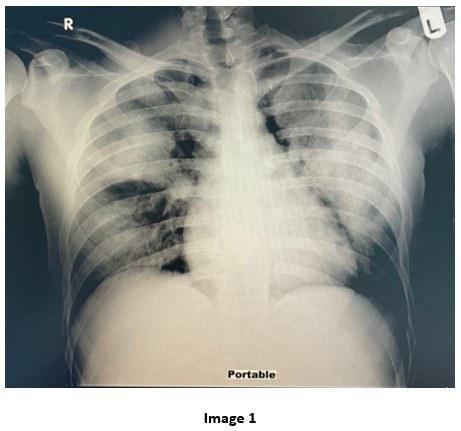
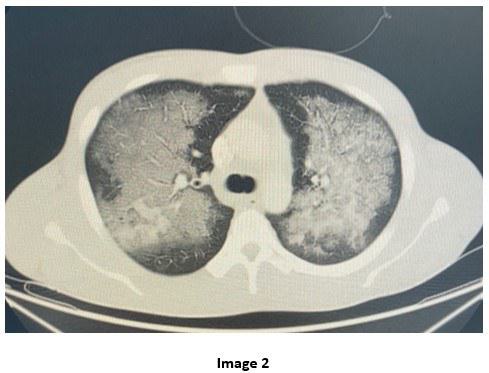
A 28-year-old male with Hepatitis C and history of substance abuse including synthetic marijuana and crack cocaine who presented with acute onset shortness of breath, hemoptysis and chest tightness of 2 hours duration. Upon evaluation, he was found to be hypoxic with SpO2= 80% on non-rebreather mask (FiO2= 100, Flow= 15L/min) requiring intubation. Complete Blood Count (CBC) revealed leukocytosis WBC= 21.13 x10 3 with neutrophilic predominance (92%) and left shifting of +1. Renal panel without major electrolyte disturbance or acid base disorders. The urine toxicology positive for Cocaine and THC. Mycoplasma IgM titers, Influenza A and B titers and Mycobacterium tuberculosis smear and culture were all negative. He was treated with systemic corticosteroid, scheduled bronchodilators and started on broad spectrum antibiotics. He was admitted to the Medical Intensive Care Unit. The chest X-ray and chest CT obtained are shown below
Question
Which of the following is the most likely causative agent of this patient’s abnormal radiological findings?
A. IV drug cocaine
B. Inhaled cocaine
C. Synthetic Marijuana inhalation
D. Reactivation of Pulmonary tuberculosis
E. Aspiration pneumonia