Author
Steven Holets RRT
Assistant Professor of Anesthesiology
Mayo Clinic College of Medicine
Case
Scenario: 76 yo man with history of COPD was admitted 3 days earlier with a diagnosis of pneumonia requiring intubation and mechanical ventilation. He is now clinically improved with antibiotics and mechanical ventilation. This morning’s ABGs Pa02 105, PaC02 44. pH 7. 41, with calculated bicarbonate of 29 were drawn while the patient was sleeping and on assist control volume ventilation Fi02 .40, RR 16, Vt 450 (6ml/Kg predicted body weight) PEEP 6 cmH20. He was subsequently switched to Pressure Support mode to evaluate for weaning with settings of Fi02 .40 pressure support 12 cmH20 and PEEP of 6 cmH20.
The patient is awake and responds to commands but appears somewhat uncomfortable and agitated. The nurse says the patient seems to be “fighting the ventilator”. Current ventilator displayed data include respiratory rate 14, spontaneous tidal volumes (Vt) of 350-600 ml, minute ventilation 9.8 liters and peak airway pressure (Paw) 18cmH20.
Vital signs: Pulse 110 beats per minute, blood pressure 120/56, Sp02 of 95%.
You observe the ventilator waveform.
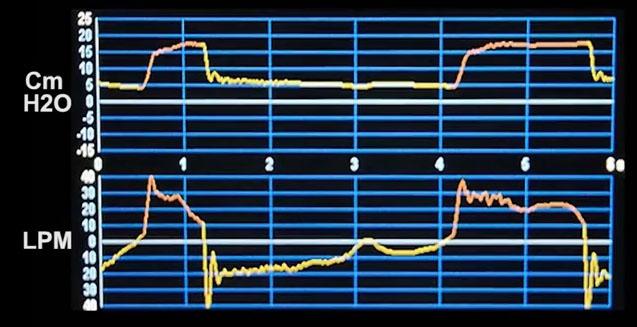
A video clip of the waveform
Question
What form of patient ventilator dysynchrony is clearly evident?
A. Delayed expiratory cycling -Prolonged inspiration due to an inappropriately high pressure support setting.
B. Inspiratory flow starvation (inadequate rise time setting).
C. Ineffective Triggering-Wasted inspiratory efforts.
D. Autotriggering –caused by occasionally cardiac artifacts.



