Answer
Brandon Janssen1, MD, Diana Gomez Manjarres2, MD, and Divya C. Patel2, DO
1Department of Medicine; University of Florida
2Division of Pulmonary, Critical Care and Sleep Medicine; University of Florida
Case

A 48-year-old woman with a reported history of sarcoidosis presented to the emergency department with worsening dyspnea on exertion, generalized fatigue, and cough productive of yellow sputum. She also reports chronic joint pain and the findings on her hands as shown.
The review of systems was negative for fevers, chills, night sweats, unintentional changes in weight, myalgias, muscle weakness, gastroesophageal reflux, and Raynaud’s phenomenon. She is a never smoker and has no relevant respiratory exposures.
Labs were significant for ESR of 121 mm/hr, CRP of 69 mg/L, CK of 381 U/L, aldolase of 9.1 U/L, ANA with a cytoplasmic pattern and a titer of 1:320, positive anti-PL12 antibody, and positive anti-SSA IgG antibody.
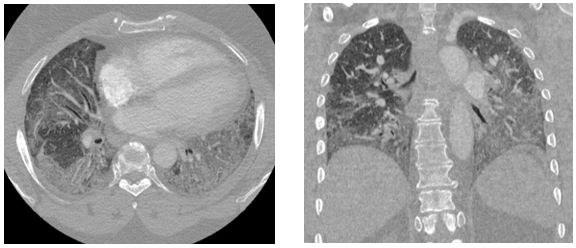
Representative images from her chest CT scan are shown below. Bronchoscopy with transbronchial biopsy and microbiological analysis were negative for evidence of infection, malignancy, and granulomatous disease.
Question
What is the most likely diagnosis?
A. Scleroderma-related ILD
B. Anti-synthetase syndrome
C. Polymyositis
D. Acute exacerbation of pulmonary sarcoidosis
E. Sjogren’s syndrome
F. Community acquired pneumonia
