Author
Burton W. Lee, MD
Pulmonary Critical Care Section
Medstar Washington Hospital Center
Associate Professor of Medicine
Georgetown University School of Medicine
Case
A 47 year-old man in the coronary care unit (CCU) presents with acute coronary syndrome and respiratory failure. Cardiac catheterization reveals severe 3-vessel disease and normal ejection fraction. Two stents are deployed. For more than a week in the CCU, patient remains intubated because of intermittent severe agitation requiring heavy sedation (Midazolam 38 mg/h, Fentanyl 75 ug/h). Patient is being considered for tracheostomy. There are no overt signs of further cardiac ischemia. Current vital signs include: blood pressure 110/65, heart rate 65, respiratory rate 28, T 98.0, urine output 100 ml/h. Patient has had a negative fluid balance of 11 liters over the past 3 days due to aggressive use of furosemide.
Current ventilator settings are Assist Control Volume Controlled Breaths; FIO2 35%; TV 0.6 l, Set Rate 12, PEEP 5, decelerating flow waveform at 30 liters/minute (0.5 liters/second). Patient’s respiratory rate is 20.
Pressure-time and flow-time curves are shown. (These are actually from another patient but the patterns were similar.)
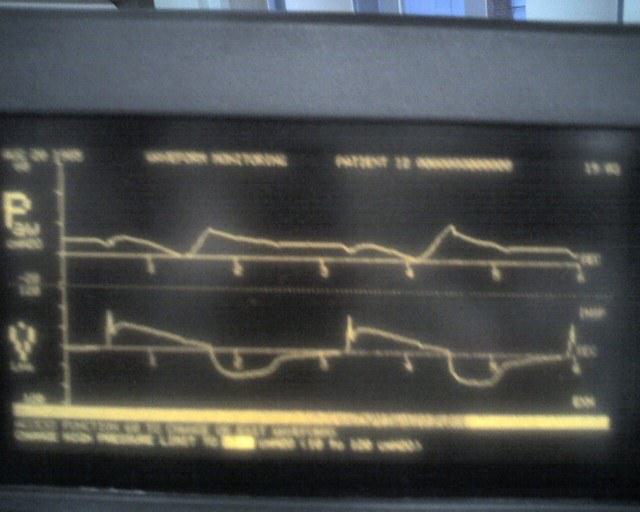
Question
Which asynchrony do the following waveforms demonstrate?
A. Premature Expiratory Cycling – Mechanical inspiratory time is shorter than the patient’s neural inspiratory time.
B. Inspiratory Flow Starvation.
C. Ineffective Triggering
D. Autotriggering